
Steelers TE Eric Ebron had one of his better games last Sunday, as Pittsburgh traveled to SoFi Stadium to face the Los Angeles Chargers. He caught all three of his targets for an average of eight yards per catch and scored his second TD of the season. Unfortunately, that TD was his final play of the game, as he was ruled out with a knee injury. Today, ESPN’s Jeremy Fowler tweeted that Ebron will likely need surgery:
Here’s the play and it’s not clear from the mechanism exactly what the injury is:
So now for some speculation on what type of knee injury Ebron sustained:
- It’s probably not an ACL tear, which is fairly easy to diagnose on physical exam alone. We would have seen one of those “the team fears the worst” type of tweets from an NFL Insider by now. Plus, Head Coach Mike Tomlin described Ebron as “questionable” to play next Sunday in his weekly media session today. As we all know, an ACL tear is season-ending.
- It’s probably not an MCL sprain. Just not a clear mechanism on video for that and isolated MCL injuries rarely require surgery unless they are severe.
- This leads me to conclude that Ebron probably sustained a meniscus tear, which can be treated operatively with an arthroscopic approach or without surgery. The twisting motion of his leg as he is tackled is consistent with that as well.
[The usual disclaimer here that I haven’t spoken with or examined Eric Ebron or seen any of his medical records]
So what if it was a meniscus tear? And what does that mean?
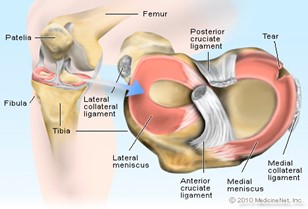
ANATOMY REFRESHER
Each knee has a medial and lateral meniscus. These crescent-shaped bands of cartilage serve as the shock absorber for the knee and allow the tibia (the larger of the lower leg bones) to glide over the bottom of the femur (thigh bone) when the knee bends. The menisci are wedges, thicker at the border where the blood supply is best and thinner in the inner aspect, which has a limited blood supply. The lateral meniscus covers a larger portion of the tibial plateau (the flat top of the tibia that articulates with the femoral condyles to form the knee joint).

A tear in the meniscus is usually caused by a quick twist or turn of the knee. As you might expect, this is a common injury in athletes. Older patients can get a tear because the tissue is old and thinned. The mechanism most likely to cause a medial meniscus tear is abduction (the leg bends out away from the body) and external rotation while bearing weight with the knee flexed. A lateral meniscus tear is caused by the opposite scenario, meaning abduction and internal rotation of a semi-flexed knee bearing weight.
There are a variety of ways the meniscus can tear:
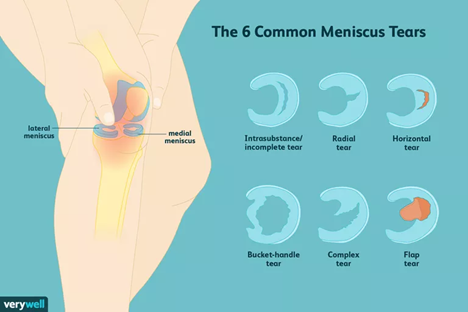
www.verywellhealth.com
Rest and physical therapy is often the first line of treatment and can be effective but not all patients can return to full physical activity without surgery. In a New Journal of Medicine study comparing PT versus surgery, patients were randomly assigned each treatment group. 33% of patients from the PT group eventually crossed over and underwent surgery. Timing may be a factor in Ebron’s decision here, since he will be a free agent after this season.
WHY DO SURGERY
If not repaired, the tear can get worse.
Ongoing pain can be eliminated.
Playing on a meniscus tear can accelerate arthritis and subsequent chronic pain.
The injury can cause knee instability and negatively impact the quality of the player’s performance.
The player may be able to achieve a faster return to play.
Meniscal tears are typically treated surgically with one of two options:
- Partial or complete meniscectomy (removal of part or all of the meniscus on the affected side)
- Repair of the meniscus by suturing the tear
Remember earlier that I mentioned only the outer, thicker border of the crescent-shaped meniscus has a good blood supply and the inner border of the meniscus is avascular? That is a factor in the choice of operation. An attempt to repair the inner rim is usually not successful because the lack of blood supply does not allow for healing the edges of the repair.
Lateral meniscus tears typically require surgical treatment to prevent both early problems and later development of chondral degeneration which affects the athlete’s performance. Medial meniscus tears are often treated surgically to achieve a faster recovery than PT and rest would provide.
RECOVERY TIME
With a partial or even a complete meniscectomy, patients are able to be full weight bearing immediately after the surgery, so no crutches are necessary unless the patient is hesitant to walk due to pain. Pain is primarily due to swelling from the initial injury and tends to be the rate-limiting step to recovery. Players will often wear a brace when first returning to practice but not to play.
The average time for all meniscus repairs is 4-6 weeks but it depends on the type of tear and the type of repair needed.
- A meniscectomy has the fastest recovery at 3-6 weeks.
- A simple meniscus repair may sideline a player for 6-20 weeks.
- A complex repair can be season-ending, taking anywhere from 7-12 months for return to play.
Lateral meniscus repair typically has a longer recovery. In a review of NFL players undergoing 77 repairs of the lateral meniscus, Dr. James Andrews found that 61% (n = 47) resulted in the athlete returning to play at his previous level of competition with an average length of time to RTP of 8.5 months. Studies show that medial meniscus repair can be much faster.
Some players come back fairly quickly as we have seen with some past Steelers:
- LB Ola Adeniyi underwent meniscus surgery prior the second preseason game and returned for the Week 2 regular season game, missing only 4 weeks.
- Benny Snell underwent meniscus surgery in late October, missing only 2 games.
- QB Ben Roethlisberger underwent a meniscus surgery in 2016, missing only 2 games in 3 weeks, returning to face the Ravens in Week 9 after the bye week.
We don’t know the type or severity of Ebron’s knee injury and the team may not provide any further detail. The veteran TE reportedly plans to seek a second opinion before going under the knife. Based on his Instagram post and the replies from his teammates, however, it’s certainly possible that he won’t be back that soon:
If the Steelers can somehow find some consistency and put together a string of wins in the coming weeks, there is still a good chance that Eric Ebron can find his way back to the 53 man roster by late December or January. If they have been eliminated from the playoffs by the time Ebron could return, there’s a good chance he has played his last snap for Pittsburgh. Let’s hope there’s a moving train worth boarding.
“Melanie H. Friedlander, M.D., F.A.C.S. is a doctor at Association of South Bay Surgeons in Torrance, California. Dr. Friedlander enjoys all aspects of general surgery, but her primary areas of focus are breast surgery and advanced laparoscopic surgery. She recently adopted an advanced, minimally invasive technique that reduces scar size in thyroid surgery. Dr. Friedlander is a member of the Society of American Gastrointestinal Endoscopic Surgeons (SAGES) and the Society of Laparoscopic Surgeons. She developed and published many scientific studies in highly esteemed medical journals.”






