Just when you thought the Steelers’ defense would be at full force, the announcement that reigning DPOY linebacker TJ Watt was activated to the active roster was coupled with the update that star safety Minkah Fitzpatrick was downgraded to out for Sunday. He reportedly developed abdominal pain during the walk-through on Saturday and subsequently underwent an appendectomy for appendicitis. As originally reported by NFL insider Adam Schefter, Fitzpatrick may miss multiple weeks:
In his article, Schefter referenced Cincinnati Bengals quarterback Joe Burrow as an example of a player missing more than two weeks of practice. Burrow was reported to have suffered a perforated appendix and was noted to have an IV in his arm when he visited training camp, suggesting that he was receiving intravenous antibiotics even after he was discharged from the hospital. While no details are available regarding the severity of Minkah’s appendicitis, there is no reason to assume that his case is similar. Let’s take a quick break to review the anatomy and the disease process and we’ll get back to Minkah’s likely return to play timeframe.
ANATOMY
The appendix is a blind end tube of intestine that extends from the first portion of the large intestine, just beyond the junction of the small and large intestines. It does not have any proven function with regard to digestion.
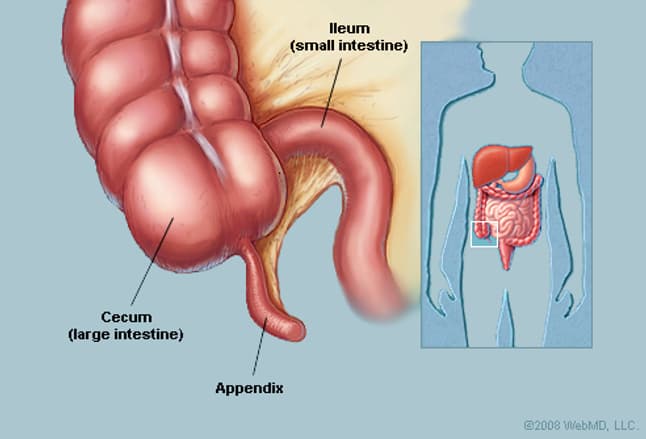
www.webmd.com
APPENDICITIS
When the appendix becomes inflamed, there are varying degrees of severity:
- Early acute appendicitis — the appendix is inflamed but there is no pus present
- Suppurative acute appendicitis — the appendix contains pus but there is no perforation
- Gangrenous appendicitis — the wall of the appendix is so inflamed that the small blood vessels in the wall are compressed, limiting perfusion and causing ischemia
- Perforated appendicitis — the wall of the appendix has ruptured, releasing pus and bacteria in the abdomen
Appendicitis is most common between the ages of 10 and 30 years old and the lifetime risk is 1 in 20 or 5%. A study from the World Journal of Surgery showed that perforated appendicitis occurred in 19% of cases but was much less common among adolescents and young adults (age range 13-40 years old). Perforation was found in higher rates in small children and the elderly. Symptoms may vary but the most typical presentation is vague mid-abdominal pain that eventually localizes/focuses in the right lower quadrant. The patient may have fever, chills, nausea or vomiting. The diagnosis is typically confirmed by a CT scan of the abdomen and pelvis. In the image below, the large intestine, which contains oral contrast, appears white and the arrow indicates the inflamed appendix on cross-section:
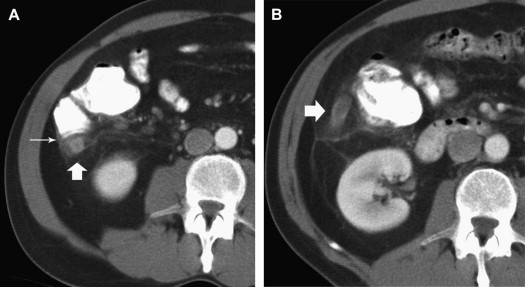
www.radiologic.theclinics.com
TREATMENT
Non-perforated appendicitis can potentially be treated with antibiotics alone. A study published in the New England Journal of Medicine randomized 1552 patients with appendicitis to surgery or a 10-day course of antibiotics. The investigators found that in the antibiotics group, appendectomy had been performed in 11% of the participants by 48 hours, in 20% by 30 days, and in 29% by 90 days; the 90-day incidence of appendectomy was 41% among those with an appendicolith and 25% among those without an appendicolith (a small stool ball in the appendix). With longer-term follow-up, the investigators found appendectomy rates in the antibiotics group were 40% one year after antibiotic therapy and 46% at two years, rising to 49% at three and four years.
SURGERY
For years, the standard treatment was the removal of the appendix through an incision in the right lower abdomen. Since the 1990s, this procedure is routinely done with a laparoscopic approach. The patient is under general anesthesia and surgery is performed through 3 tiny incisions. The surgeon inserts a telescope that is 5 mm (1/5 inch) in diameter through one of the incisions with a camera attached on the outside, showing everything in the abdomen on a video monitor. Skinny instruments are placed through the other two incisions to disconnect and remove the appendix.
For those that aren’t squeamish about surgery, here is a video of an actual laparoscopic appendectomy from Dr. Gajendra Singh, who performs the procedure the same way that I do. You are seeing the same view that the surgeon would see on the video screen. Laparoscopic removal of the appendix is one of the most common emergency procedures done by general surgeons. It typically takes me about 20 minutes from incision to skin closure. If the patient has an acute appendicitis, they often go home from the hospital the same day. Hospital stay depends on the severity of the infection and the need for antibiotics.
Here is an example from the European Journal of Pediatric Surgery that shows the standard port sites and the incisions after completion of the procedure:
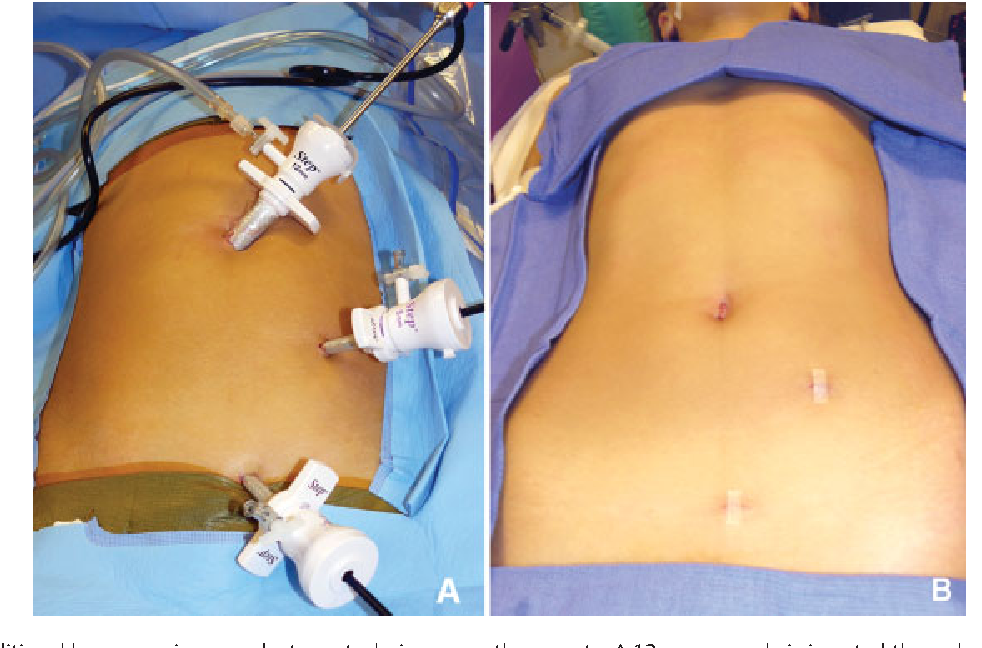
https://www.thieme-connect.de/products/ejournals/abstract/10.1055/s-0032-1320015
RECOVERY
In my practice, the typical recovery time is one week. For patients with a desk job, they usually return to work at that point. For patients with a physical job, they are cleared for full activity but may not feel ready. Obviously, what NFL athletes do on the field cannot be compared to the weekend warriors in my practice.
Where NFL players are concerned, there is no published data on return to play. Steelers fans will recall that in 2002, wide receiver Hines Ward underwent an emergency appendectomy during the preseason. His surgery was performed on a Friday night, he was discharged from the hospital the following day, and he returned for the Week 2 game three weeks later. In 2006, quarterback Ben Roethlisberger had an appendectomy three days prior to the Thursday night season opener and was able to start 14 days later in Week 2.
Considering the short time from onset of symptoms to surgery for Minkah, he most likely had a straightforward acute appendicitis. It’s also a great sign that he was present on the sideline Sunday and moving around comfortably just one day after surgery. Assuming that is the case, he could return to practice next week. It is extremely unlikely that he would be ready to play next Sunday when the Steelers take on the Bengals but there is a very good chance that Fitzpatrick could be back for the Monday Night Football game against the Indianapolis Colts in Week 12. I would expect him back for the following week against the Falcons at the latest.
“Melanie H. Friedlander, M.D., F.A.C.S. is a doctor at Association of South Bay Surgeons in Torrance, California. Dr. Friedlander enjoys all aspects of general surgery, but her primary areas of focus are breast surgery and advanced laparoscopic surgery. She recently adopted an advanced, minimally invasive technique that reduces scar size in thyroid surgery. Dr. Friedlander is a member of the Society of American Gastrointestinal Endoscopic Surgeons (SAGES) and the Society of Laparoscopic Surgeons. She developed and published many scientific studies in highly esteemed medical journals.”