
In the two days since a wild Steelers win over the Bengals, the news regarding defensive star OLB TJ Watt has been something of a roller coaster. Walking off the field with mere seconds left in the 4th quarter, Watt looked distressed as he pointed to his left chest and appeared to say that he tore it. Steelers fans were devastated at the thought of losing this one-man wrecking crew to a season-ending injury. But as updates came from NFL insiders Ian Rapoport and Adam Schefter, it seemed that maybe there was hope Watt’s season wasn’t a total loss. Let’s take a look at what we know so far.
THE ANATOMY
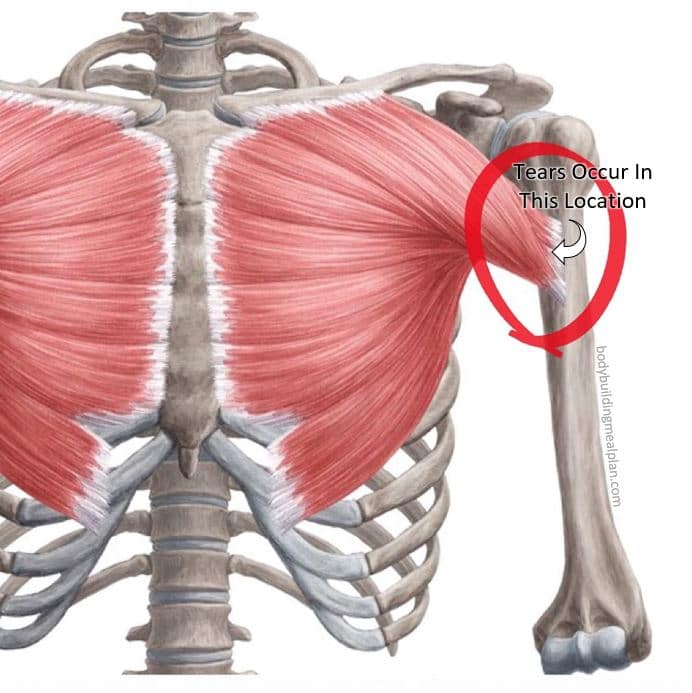
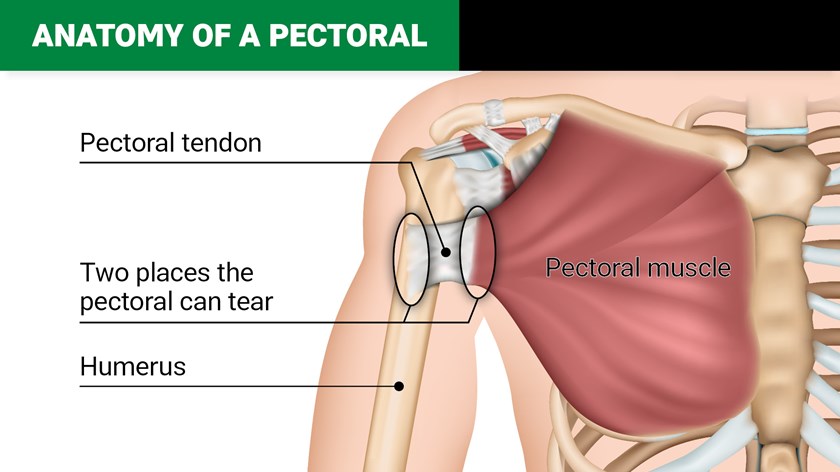
The pectoralis major muscle originates on the sternum (breastbone) and the clavicle (collar bone). It cover the rib cage and inserts, or attaches to, the humerus (the long bone of the upper arm). A tendon attaches the muscle to the humerus.
www.bodybuildingmealplan.com
The pectoralis major may tear or rupture in various parts of the muscle. Most pectoral injuries involve a rupture of the tendon off the humerus bone. There appears to be a correlation between the mechanism of injury and site of rupture. Tears of the muscle belly are more common with direct trauma. Indirect trauma leads to tearing of the muscle from the tendon or the tendon from the bone. The muscle can also tear off the sternum, which is really rare.
When a pectoral tear occurs in an NFL player, it typically involves the tendon that attaches the muscle to the humerus – either the muscle tears from the tendon or the tendon tears from the bone. Either tear can be partial, like a frayed rope, or complete.
www.nrl.com
THE INJURY
Watt knew immediately that something was wrong. With a pectoralis tear, a sudden sharp pain is common and sometimes there is an audible popping sound as well. In the play where he was injured, you can see his left arm across Bengals QB Joe Burrow’s back. As Watt falls, his left arm is extended:
In the locker room, trainers would have examined Watt for left arm range of motion and palpated the muscle to see if it had retracted from the left humeral bone. At this point, they already may have had reason to be optimistic that the tear was not severe. With a full tear of the tendon, the muscle can visibly retract onto the chest:

www.sciencedirect.com
Watt had an MRI the following day and was evaluated by the team doctor. After that, he was reported to be in team meetings and with his teammates in the locker room. According to fellow OLB Alex Highsmith as well as several beat reporters, Watt was in good spirits. While he generally known to have a good outlook on life, this also suggests that the news he received was somewhat encouraging.
Later in the day, the news cycle continued. Watt would be seeing a second and third opinion regarding his treatment plan. This suggests that the tear isn’t so significant that he absolutely needs surgical repair but that it isn’t minor enough that surgery is not definitely needed.
SURGICAL REPAIR
If the tendon has been torn away from the bone, surgical treatment is recommended, especially when it involves high-level athletes. Surgery yields excellent results as far as return to pre-injury strength.
The repair is performed through an incision on the upper arm, and the tendon is anchored to the humerus. When the tendon has torn off the bone, that is the most straightforward repair. The tendon is secured to the bone with sutures. When the muscle tears from the tendon, the repair is more difficult, as the muscle fibers don’t hold the suture well. A variety of techniques have been developed to secure the muscle back to the tendon.
You can see an animated version of a pectoralis tendon repair here, courtesy of Dr. Howard Luks.
NON-OPERATIVE MANAGEMENT
For partial tears of the muscle, surgery is usually not needed. As you can imagine, suturing muscle fibers doesn’t really provide any benefit, as the suture material will just pull through the muscle. The muscle fibers will heal over time without surgery.
So what about return to play if no surgery is needed? We have an example from 2020. In the season opener against the New York Giants, Right Guard Stefen Wisniewski was filling in for an injured David DeCastro and sustained a pec injury. He was placed on injured reserve but was cleared to return to practive on October 14, exactly 4 weeks after his injury. He was activated prior to the 21 day deadline but was released 3 days later and then signed by the Kansas City Chiefs. The general consensus at the time was that Wiz had recovered well but that the Steelers let him go because the team had greater roster needs at other positions.
RECOVERY TIME
If you were on Twitter in the past day, you probably saw a variety of predictions on return to play for TJ Watt, ranging from four to six weeks without surgery and four to six months with surgery. The bottom line is that players get back on the field a lot faster when they can bypass the OR. A 2019 review of NFL players treated for pec injuries over 15 seasons found 132 strains and 79 complete ruptures. Of the players with strains, only 10 required surgery and the mean return to play for those treated with rehab alone was only 28 days. The 52 players with complete ruptures who required surgery had a mean return to play of 147 days.
A 2021 study looked at PFF rankings of NFL players before and after repair of pectoralis injuries. 79% of the 63 players with pectoralis ruptures reviewed were defensive players. Over 85% of the players returned within one year of injury. There was no statistically significant decrease in the PFF grades for any player evaluated. Linebackers averaged a PFF grade of 63.5 prior to injury and 61.4 following return from surgery.
SPECULATION TIME
Obviously, I have no access to TJ Watt’s medical records or any inside knowledge. This are just my conclusions based on everything that has been reported. Watt most likely has a partial tear that does not involve the attachment of the pectoral tendon to his humerus (or he would already be scheduled for surgery). And I would guess that the tear is more than just a Grade 1 that would clearly heal without surgery but not so significant that surgery is absolutely necessary.
When a player sees three surgeons prior to making a decision on whether to undergo a procedure, it tells me that the case requires a judgment call. And given that the decision involves the reigning Defensive Player of the Year, that becomes all the more difficult. When weighing the pros and cons, TJ and his doctors have to consider his long-term outlook and recovery as well as his ability to get back on the field this season. As much as he wants to rejoin his teammates and play out the season, he may be better served by undergoing a surgical repair now.
Based on what we heard late yesterday, it sounds as though Watt is leaning towards a course of rehab with the hope of a quick return. Whatever his treatment course, he will almost certainly go on the Reserve/Injured list with a plan to return after missing the required minimum of four games. Hopefully, he will make it back to torment opposing quarterbacks again this season.
“Melanie H. Friedlander, M.D., F.A.C.S. is a doctor at Association of South Bay Surgeons in Torrance, California. Dr. Friedlander enjoys all aspects of general surgery, but her primary areas of focus are breast surgery and advanced laparoscopic surgery. She recently adopted an advanced, minimally invasive technique that reduces scar size in thyroid surgery. Dr. Friedlander is a member of the Society of American Gastrointestinal Endoscopic Surgeons (SAGES) and the Society of Laparoscopic Surgeons. She developed and published many scientific studies in highly esteemed medical journals.”






